What is ABA?
But first, what is behaviour?
Something that can be, objectively defined, accurately measured, and easily observed.
Does it pass the dead mans test? Only a living organism can emit behaviour

Functional Behaviour Assessment – understanding functional relationships
We use a variety of methods to understand WHY a behaviour may be occurring.
Why are these methods helpful?
EXAMPLE: ABC analysis (antecedent, behaviour, consequence)
what happens before, during, and after a behaviour
Whenever I see a bag of Reece’s mini’s, I stop and eat the whole thing!
Antecedent: I see the bag of chocolate in my pantry.
Behaviour: I eat the whole bag.
Consequence: The chocolate taste delicious! I know this wasn’t a healthy choice.
This problem could easily be remedied through an antecedent strategy. You guessed it…don’t buy chocolate.
BUT chocolate is my roommates’ favourite – so I can’t not buy it. How else can we change the environment to help me with this problem?
A: I put a visual representation of my fitness goals next to the chocolate in the pantry. Some people choose pictures of themselves, others may write a specific weight goal, etc.
B: I go to get chocolate and I see the visual. I decide not to eat the chocolate.
C: I put a dollar in my “good decision” jar, which can be cashed in for new clothes every week!
By changing the environment and adding a reinforcing consequence (rewarding myself with a dollar) for a good decision, I have changed a bad habit!
References:
Cooper, J. O., Heron, T. E., & Heward, W. L. (2019). Applied Behavior Analysis (3rd Edition). Hoboken, NJ: Pearson Education.
Autism Spectrum Disorder (ASD) is a neurological and developmental disorder associated with these symptoms:
Symptoms of ASD typically appear in the first two years of life.
ASD is known as a “spectrum because there is wide variation in the type and severity of symptoms people experience.
Social Communication/interaction behaviours may include:
Restrictive/Repetitive behaviours may include:
Some strengths may include:
Supporting someone with ASD
Think of fun things to do that keep in mind the sensory sensitivities specific to the person and schedule time to enjoy being with them.
References:
Autism spectrum Disorder. (n.d.). National Institute of Mental Health (NIMH).
https://www.nimh.nih.gov/health/topics/autism-spectrum-disorders-asd
Signs & Symptoms | Autism Spectrum Disorder (ASD) | NCBDDD | CDC. (2023, January 11). Centers for Disease Control and Prevention.
What is autism spectrum disorder? (n.d.).
https://www.psychiatry.org/patientsfamilies/autism/what-is-autism-spectrum-disorder
A Behaviour Support Plan is a document that is based on a written functional assessment of the person that considers historical and current, biological and medical, psychological, social and environmental factors (a bio-psycho-social model) of the person with a developmental disability that outlines intervention strategies designed to focus on the development of positive behaviour, communication and adaptive skills.
(QAM, s.15(2) definitions)
The written functional assessment refers to a detailed analysis of the behaviour relative to the environmental factors at play and as a best practice should be based on direct observation and data (as described above – although with behaviours more complex than eating Reese’s minis).
Positive Behaviour Intervention
a) Teaching or learning components, including teaching proactive skills and communication strategies to maximize the person’s abilities and to minimize challenging behaviour.
b) Reinforcement.
c) A review of the person’s living environment, including the physical space, and support and social networks, to identify possible causes of challenging behaviour and making changes to the living environment to reduce or eliminate those causes. (QAM, s.15 (5))
Intrusive Behaviour Intervention
Prescribed medication to assist the person in calming themselves, with a clearly defined protocol developed by a physician as to when to administer the medication and how it is to be monitored and reviewed (QAM, s.15(4))
References:
Ministry of Community and Social Services. (2017). BEHAVIOURAL SUPPORT PLAN
REFERENCE GUIDE for ADULT DEVELOPMENTAL SERVICES. In Ontario Regulation 299/10 Quality Assurance Measures (QAM) and the Policy Directives for Service Agencies.
https://www.mcss.gov.on.ca/documents/en/mcss/developmental/EN_BSP_REFERENCE.pdf
Bipolar disorder is a mental illness that causes unusual shifts in mood, energy, activity levels, concentration, and the ability to carry out day-to-day tasks.
Bipolar disorder is typically diagnosed during late adolescence (teen years) or early adulthood. Occasionally, bipolar symptoms can appear in children. Although the symptoms may vary over time, bipolar disorder usually requires lifelong treatment. Following a prescribed treatment plan can help people manage their symptoms and
improve their quality of life.
Types of bipolar disorder
Sometimes a person might experience symptoms of bipolar disorder that do not match the three categories listed above, and this is referred to as “other specified and unspecified bipolar and related disorders.”
The table below provides list of manic and depressive symptoms
| Symptoms of a Manic Episode | Symptoms of a Depressive Episode |
|---|---|
| Feeling very up, high, elated, or extremely irritable or touchy | Feeling very down or sad, or anxious |
| Feeling jumpy or wired, more active than usual | Feeling slowed down or restless |
| Decreased need for sleep | Trouble falling asleep, waking up too early, or sleeping too much |
| Talking fast about a lot of different things (“flight of ideas”) | Talking very slowly, feeling unable to find anything to say, or forgetting a lot |
| Racing thoughts | Trouble concentrating or making decisions |
| Feeling able to do many things at once without getting tired | Feeling unable to do even simple things |
| Excessive appetite for food, drinking, sex, or other pleasurable activities | Lack of interest in almost all activities |
| Feeling unusually important, talented, or powerful | Feeling hopeless or worthless, or thinking about death or suicide |
The table below outlines the major symptoms for a manic episode and appropriate interventions:
| Symptom | Presentation | Presentation Intervention |
|---|---|---|
| Inflated self-esteem or grandiosity | Unusually positive outlook about self, the future, and surroundings. False sense of well-being, highly confident. | Orient client to reality |
| Decreased need for sleep | Feeling rested after only a few hours of sleep. | Promote sleep hygiene - providing routine meals and sleep schedule. Provide sleep aid medication if ordered. |
| Talkative | More talkative than usual or pressure to keep talking. | Allow client to communicate as needed. Request for client to speak slowly, and repeat request as a reminder during conversations |
| Flight of ideas | Speaks rapidly about multiple subjects and experiences racing thoughts. | Provide focus for the client during conversations. |
| Distractibility | Attention is easily drawn to unimportant or irrelevant external stimuli. | Repeatedly redirect to important stimuli as needed. |
| Goal-directed | in goal-directed activity (either socially, at work/school, or sexually) or psychomotor agitation (purposeless non-goal-directed activity). Excessive involvement in activities that have a high potential for painful consequences (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments). | Set limits, boundaries, and redirection. Redirect to more appropriate behaviors. Promote a different, more appropriate activity, such as exercise. |
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Bipolar Disorder. Ontario Tech University.
Borderline personality disorder is a mental illness that severely impacts a person’s ability to regulate their emotions. This affects the way someone thinks and feels about themselves and others. This causes problems with functioning in everyday life.
Individuals with borderline personality disorder have an intense fear of abandonment, instability and may have difficulty tolerating being alone.
They may experience inappropriate anger, impulsiveness, frequent mood swings, may push others away even though they want to have loving and lasting relationships.
Borderline personality disorder typically begins in early adulthood.
Symptoms:
References:
Borderline Personality Disorder (BPD). (n.d.). CAMH.
https://www.camh.ca/en/health-info/mental-illness-and-addictionindex/borderline-personality-disorder
Cluster B disorders. (n.d.). Psychology Today.
https://www.psychologytoday.com/ca/basics/cluster-b
MindYourMind. (2016, October 13). Personality Disorders – Cluster B –
https://mindyourmind.ca/mental-health-wellness/personality-disorders-clusterb/
“Dementia is not a specific disease but is rather a general term for the impaired ability to remember, think, or make decisions that interferes with doing everyday activities. Alzheimer’s disease is the most common type of dementia.
Though dementia mostly affects older adults, it is not a part of normal aging.” (CDC, 2019).
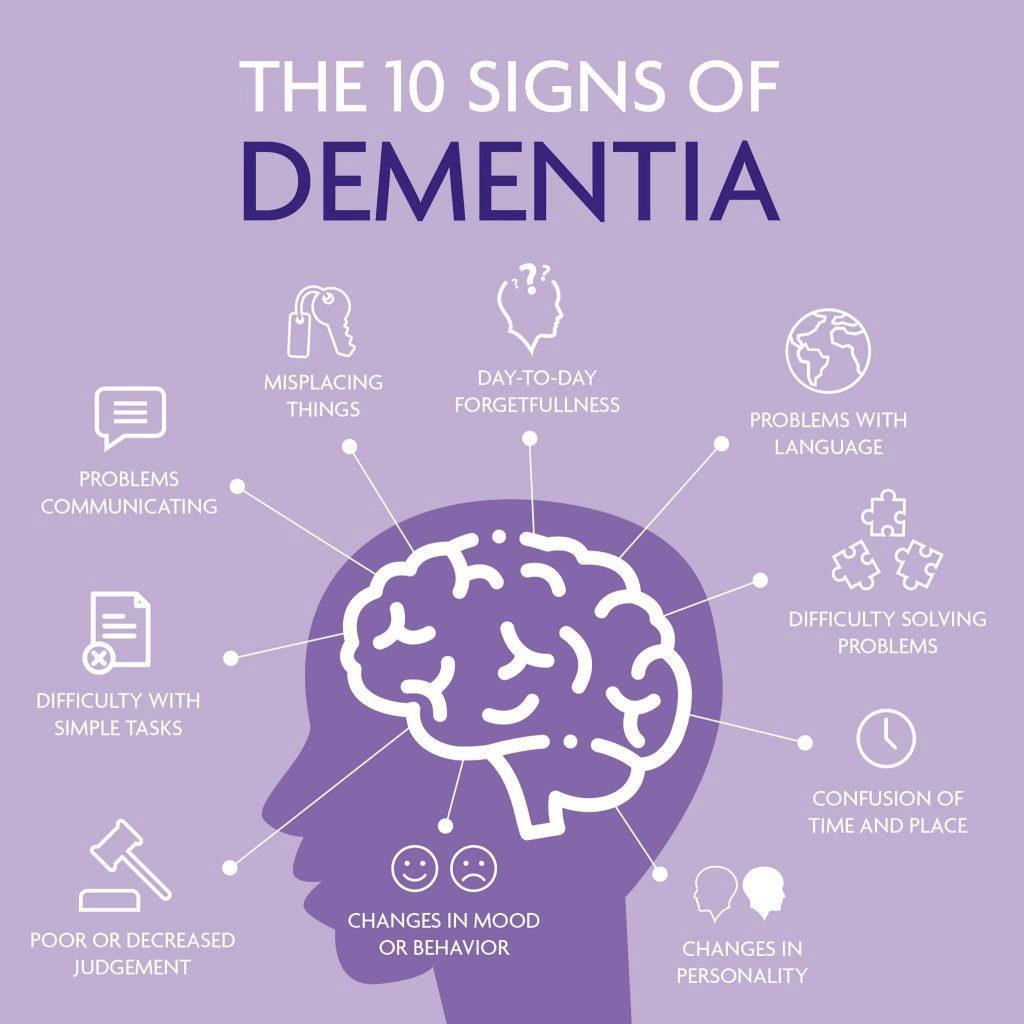
Image from: What are the symptoms of dementia How is it diagnosed. (2022). Dementia Talk Club. https://dementiatalkclub.weebly.com/blog/what-are-the-symptoms-of-dementiahow-is-it-diagnosed
What are the signs and symptoms of dementia?
Because dementia is a general term, its symptoms can vary widely from person to person. Some signs that may point to dementia include:
Environmental Strategies:
Maintaining Skills:
Coping with Sundowning (a state of confusion occurring in the late afternoon and spanning into the night)
Being too tired can increase late-afternoon and early-evening restlessness.
Try to avoid this situation by helping Client:
Avoid things that seem to make sun downing worse:
References:
Tips for coping with sundowning. (2017, May 17). National Institute on Aging.
https://www.nia.nih.gov/health/alzheimers-changes-behavior-andcommunication/tips-coping-sundowning
Understanding and supporting a person with dementia. (2022, June 27). Alzheimer’s Society.
https://www.alzheimers.org.uk/get-support/help-dementiacare/
understanding-supporting-person-dementia
What is dementia? | CDC. (2019). https://www.cdc.gov/aging/dementia/index.html
Definition: Down syndrome is a genetic disorder where the individual is born with an extra chromosome (47 instead of 46). This extra chromosome causes physical and developmental delays and disability. Physical characteristics Include: pronounced folds of skin in the inner corners of the eye, almond shaped eyes that slant up, wide set eyes
flattened appearance of the face, large protruding tongue, short stature and small ears.
Common developmental and health concerns:
Supporting someone with Down syndrome:
References:
Baksi, L. & Symbol UK. (2005). Supporting people who have Down syndrome to overcome communication difficulties (pp. 2–4).
https://downsyndromedevelopment.org.uk/wpcontent/
Down Syndrome Resource Foundation. (2022, May 9). Frequently asked questions – Down Syndrome Resource Foundation.
Stumbo, E. (2014, January 14). A closer look at the physical characteristics of Down syndrome
– Ellen Armendáriz Stumbo. Ellen Armendáriz Stumbo.
https://www.ellenstumbo.com/closer-look-physical-characteristics-down-syndrome/
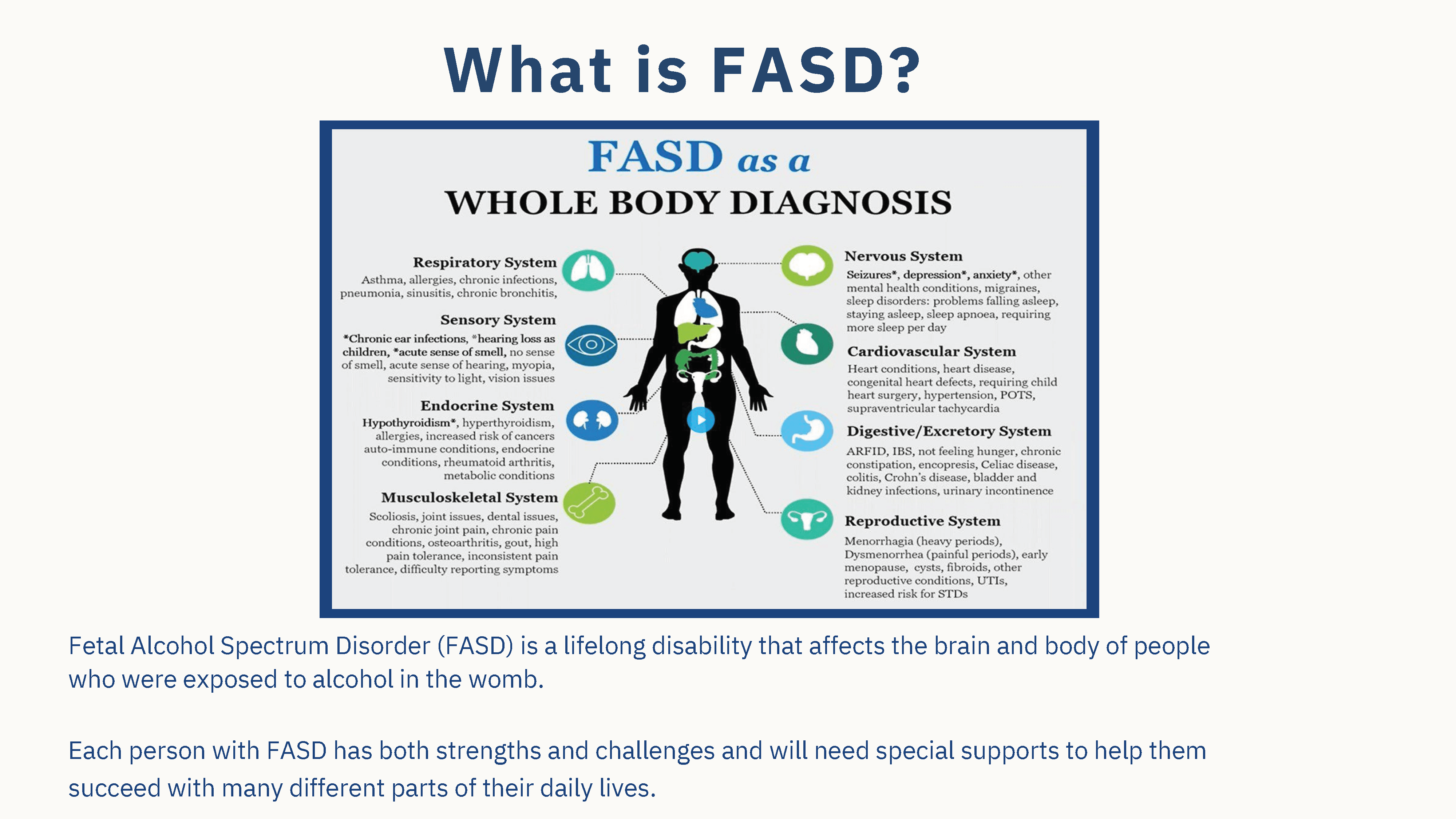
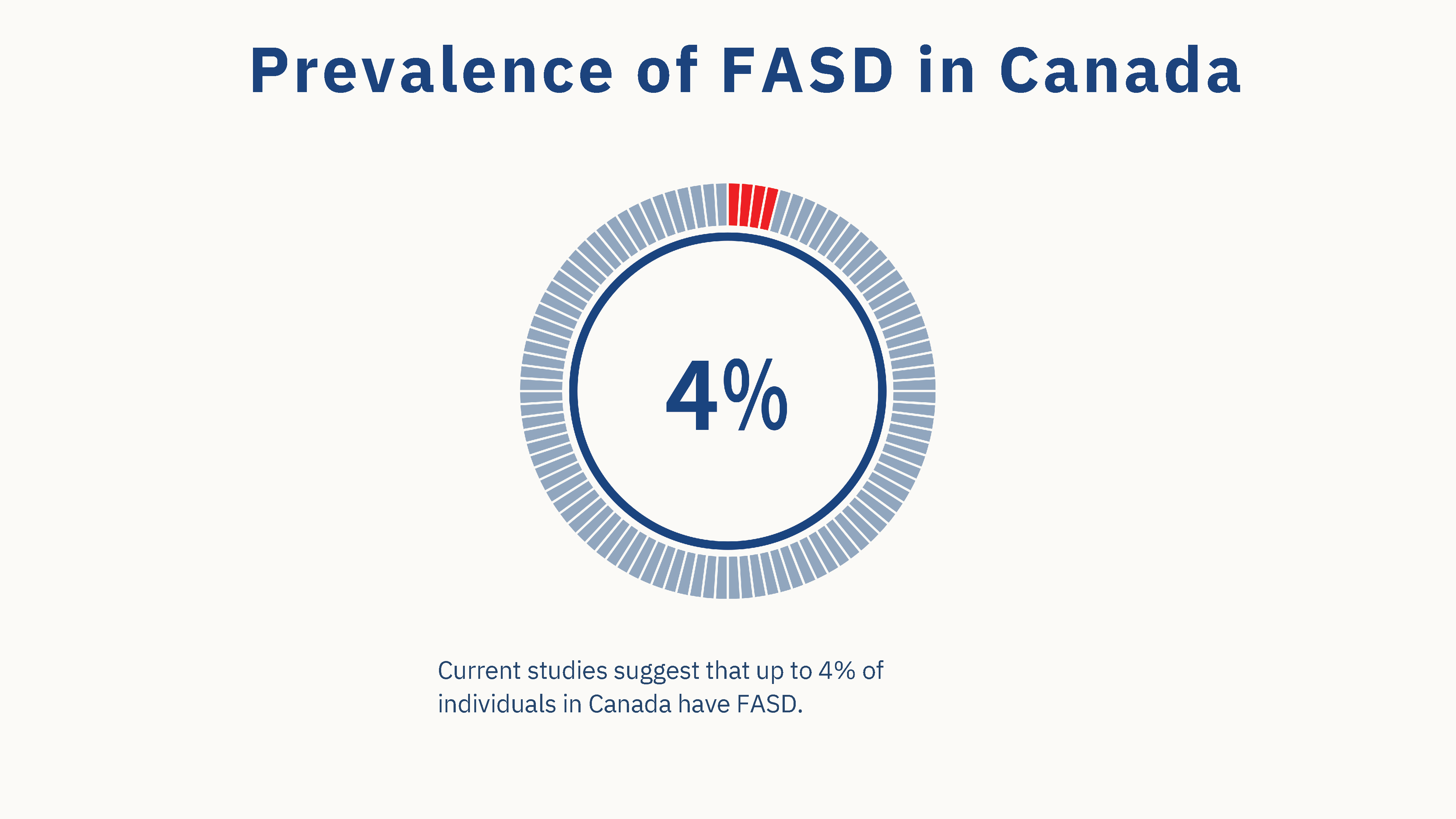
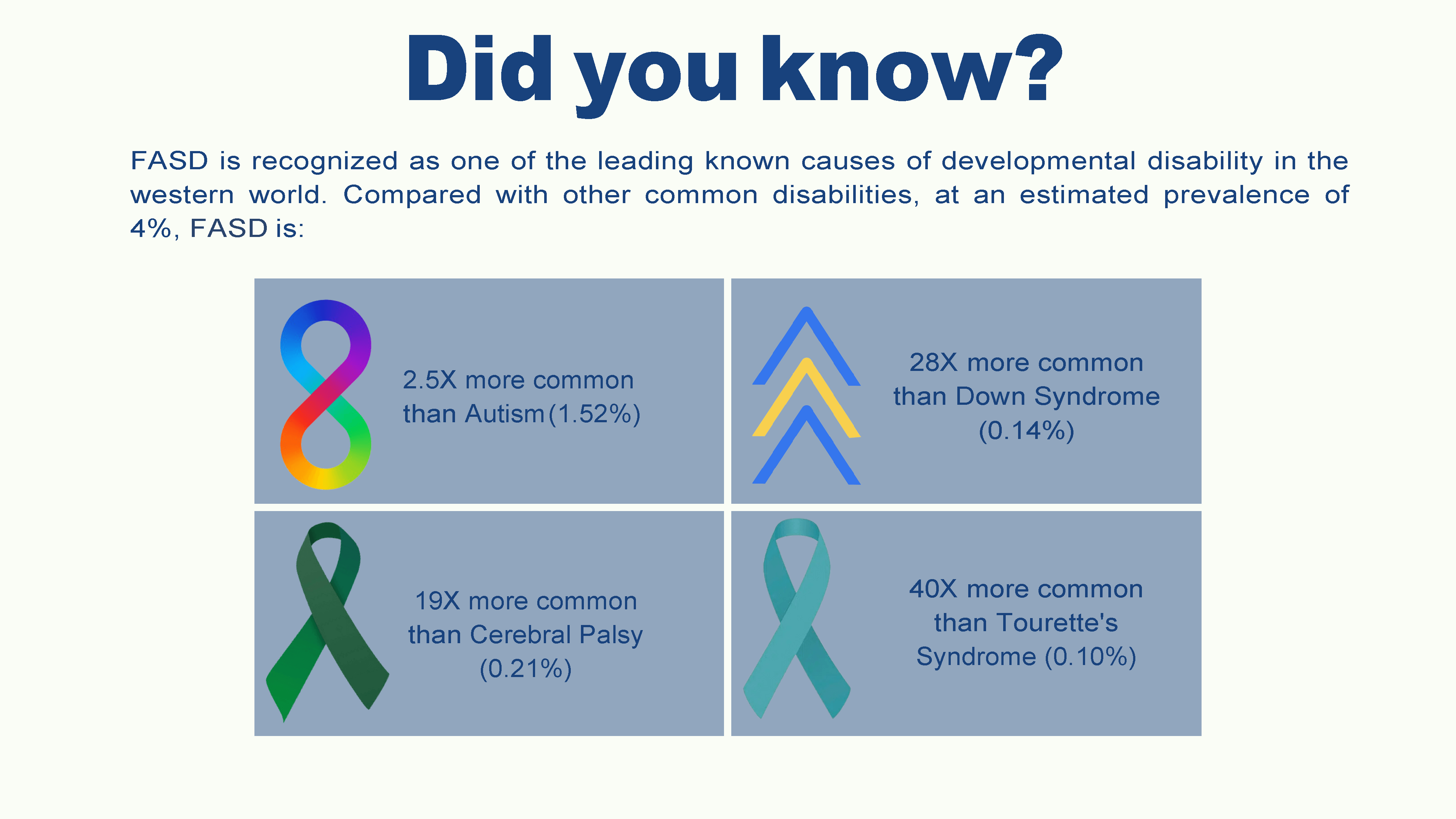
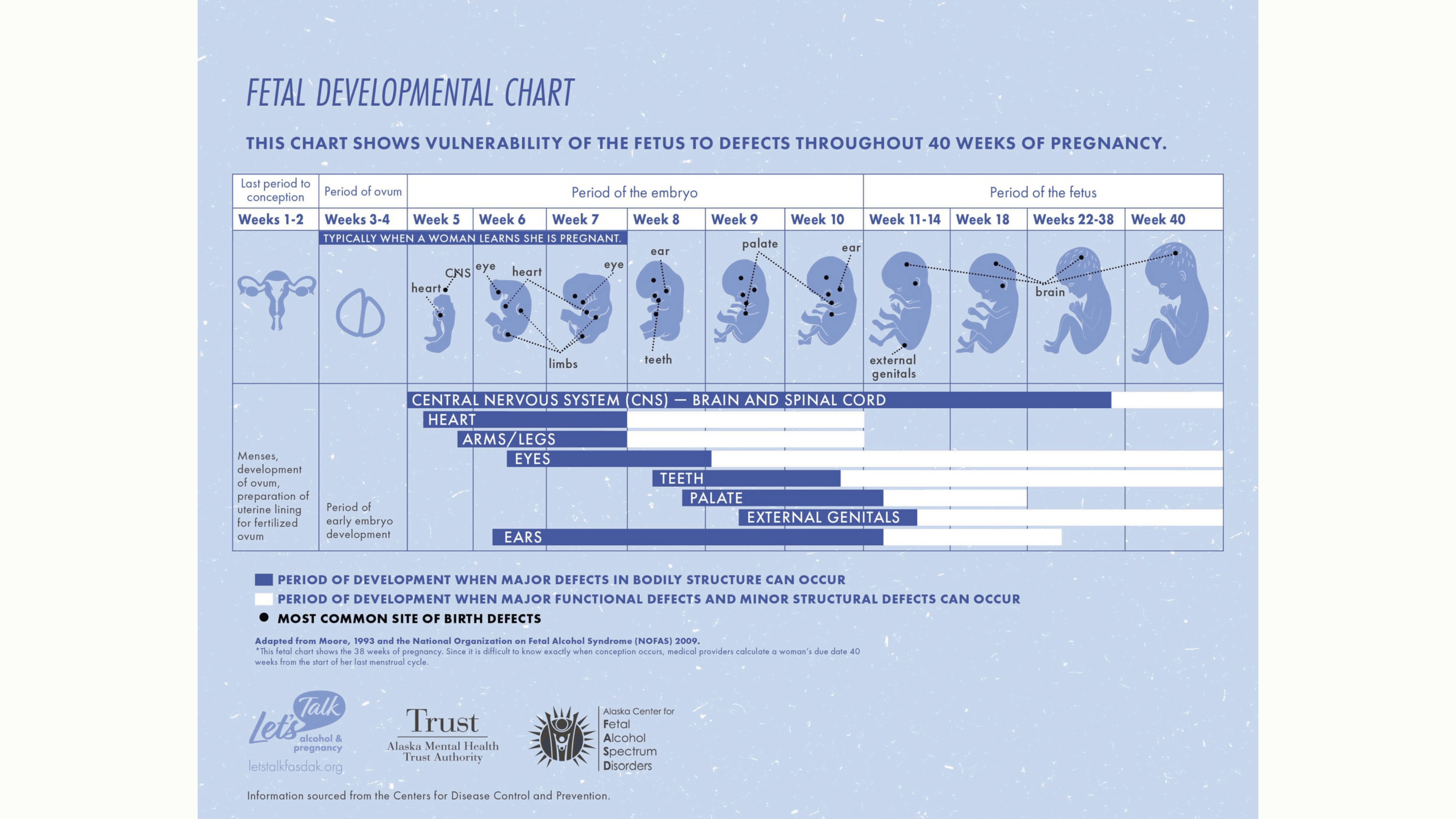
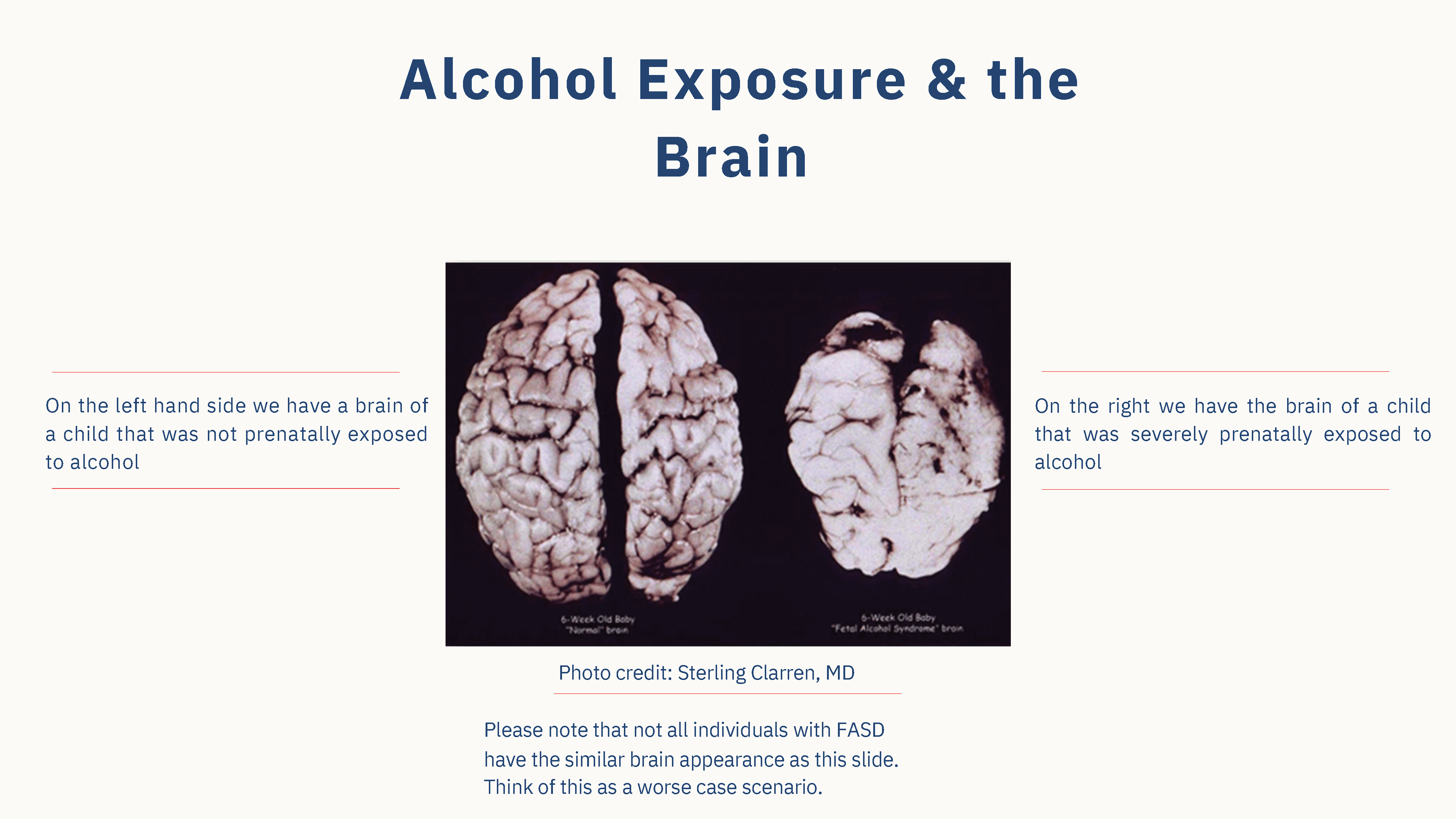
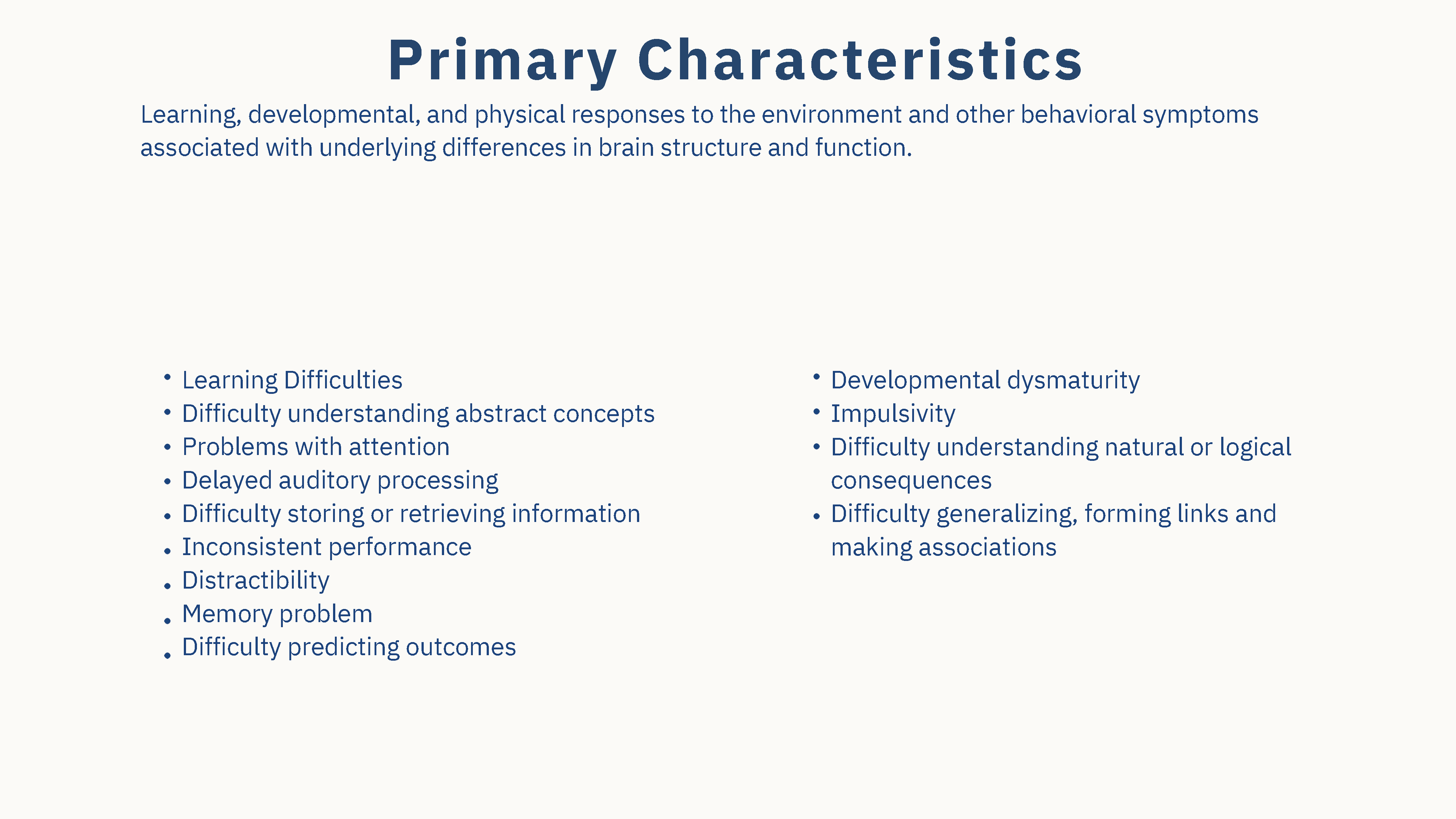
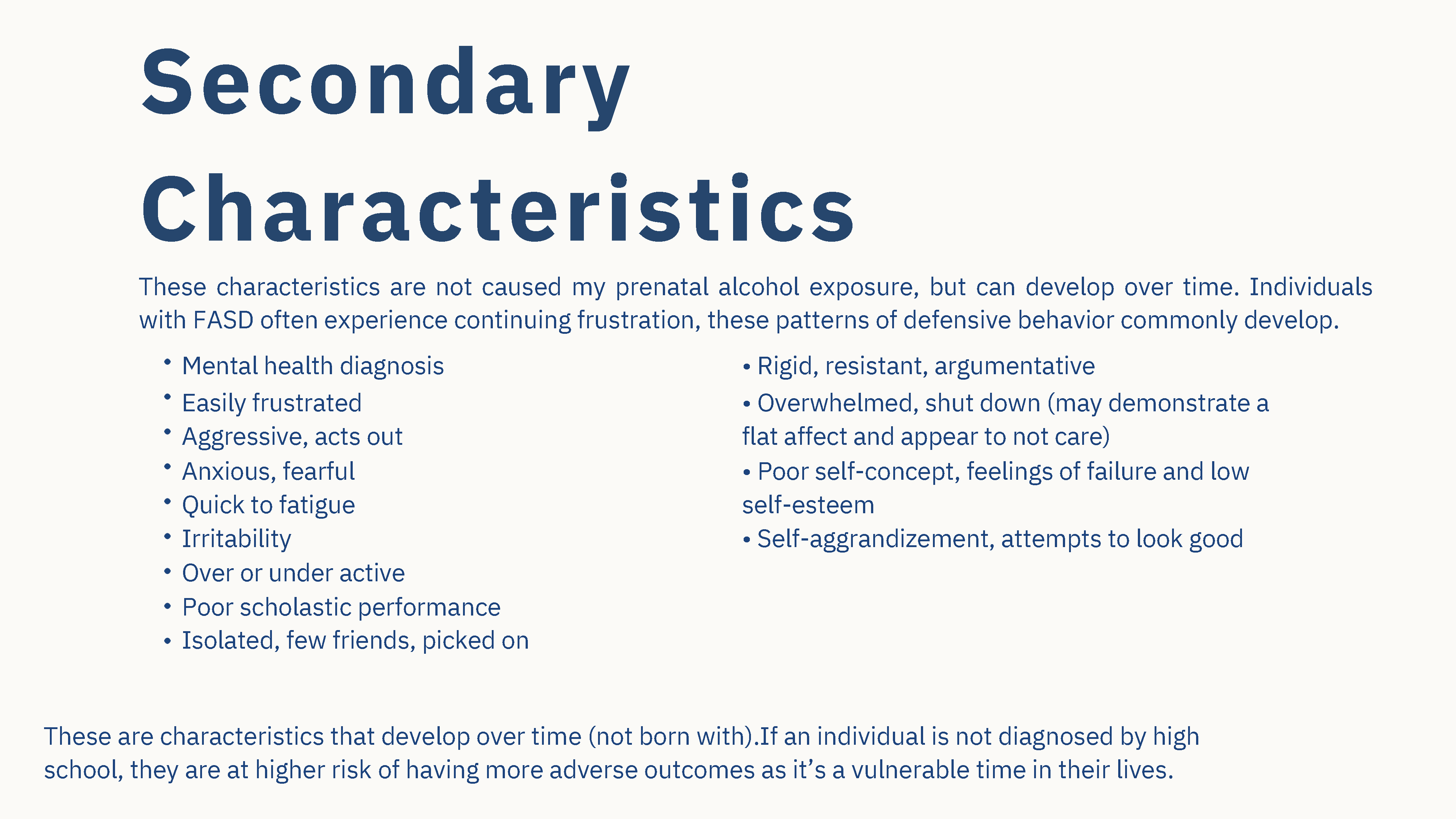
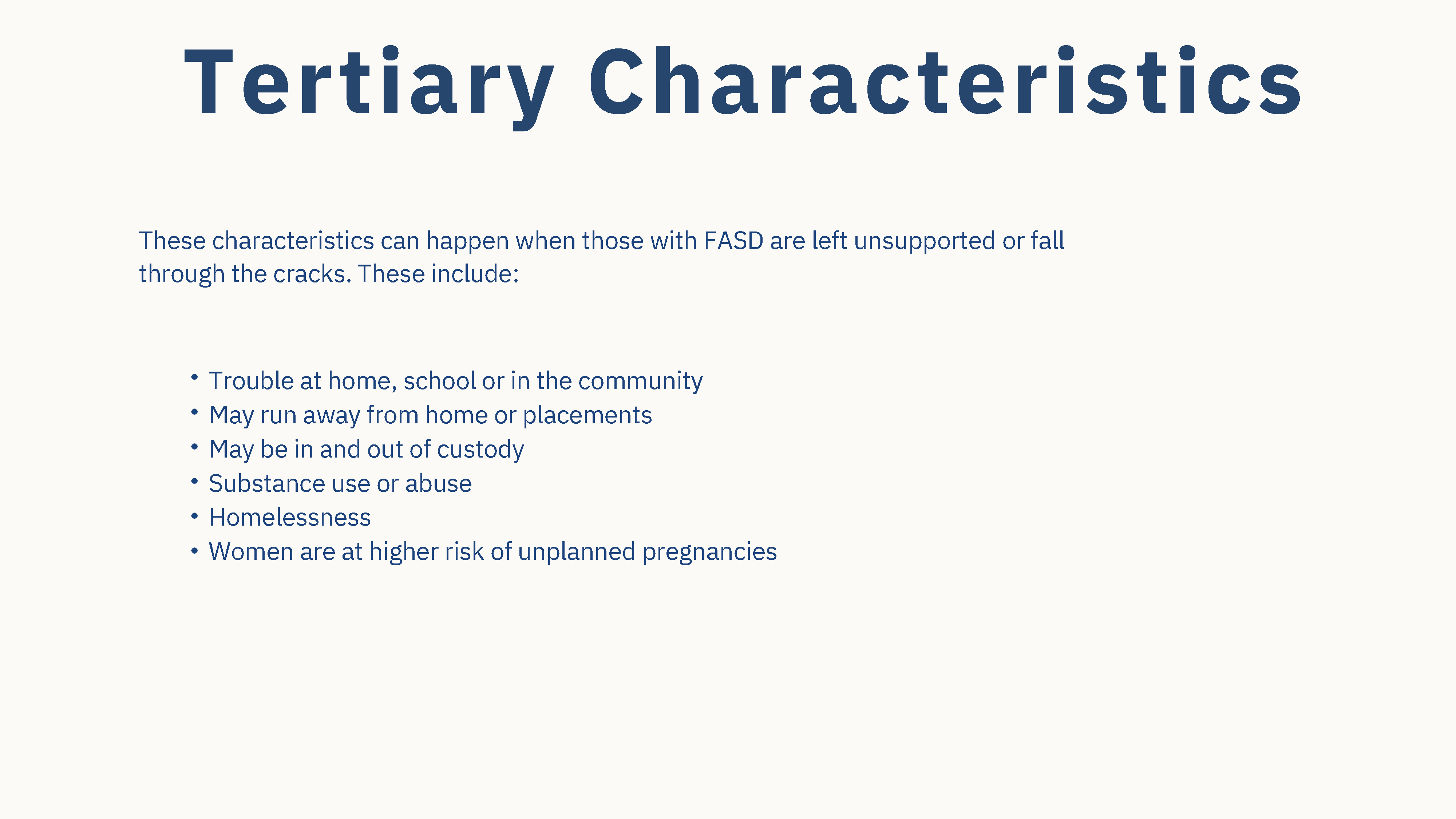
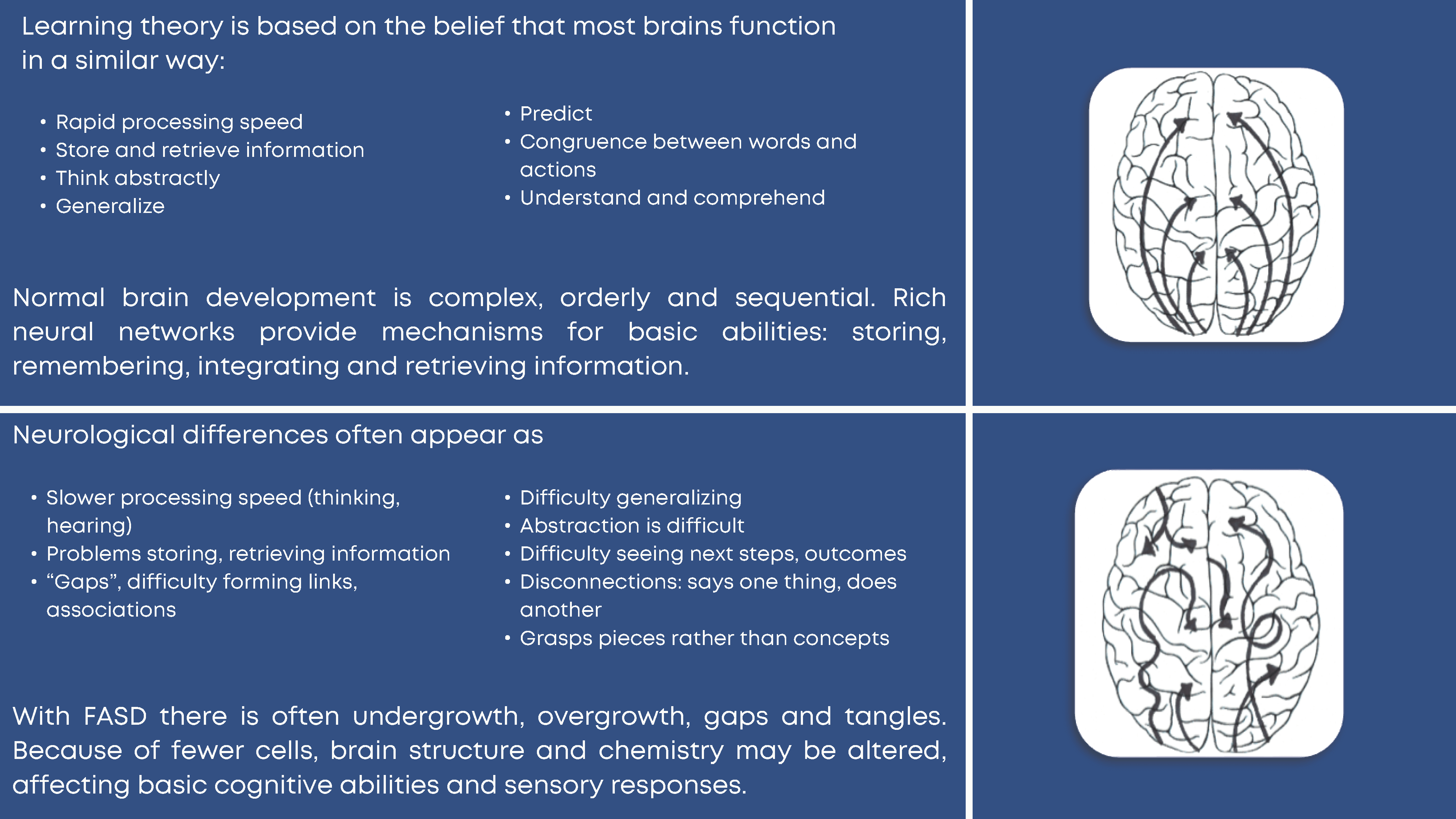
Please find the following resources for this section below:
References:
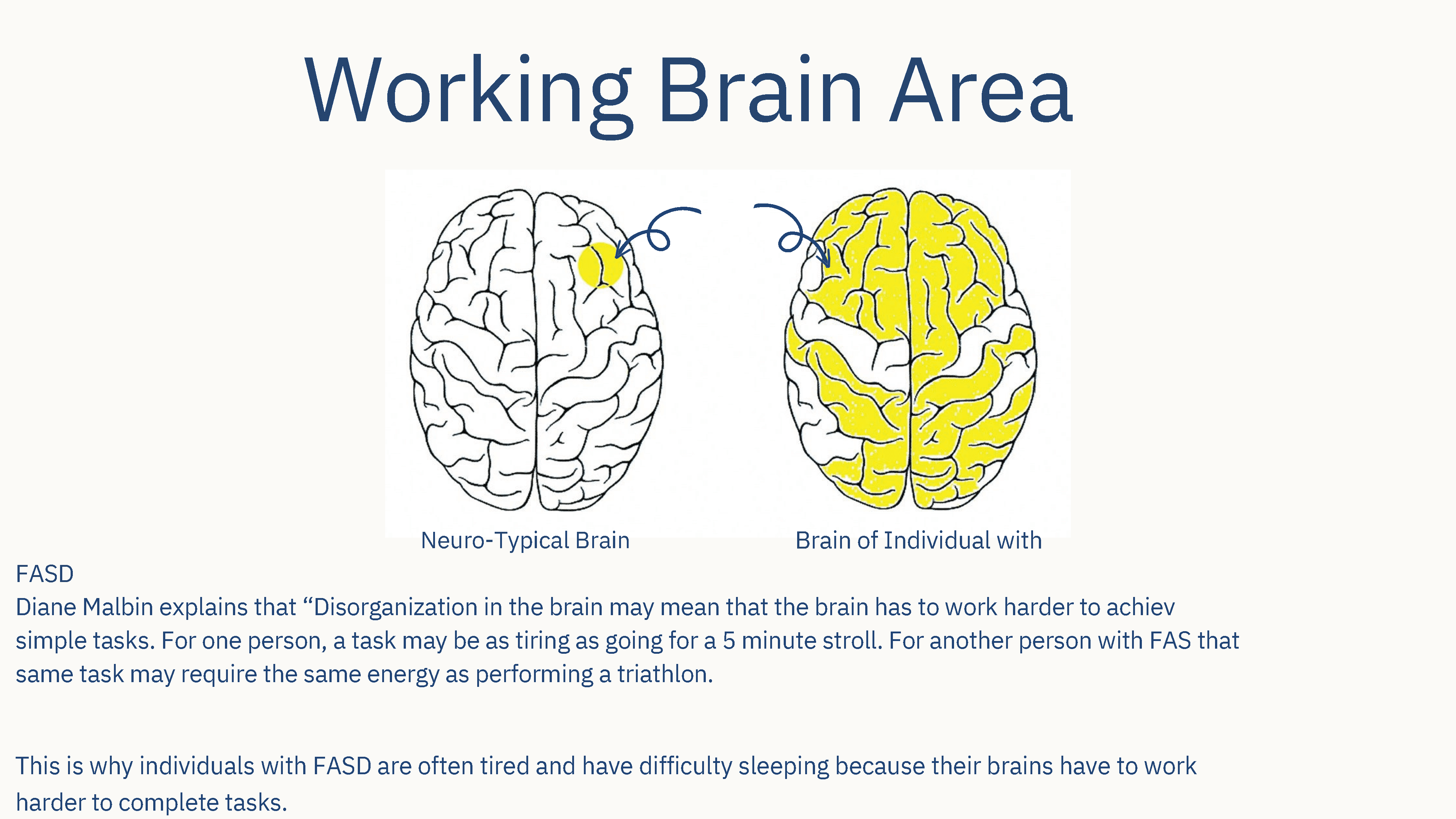
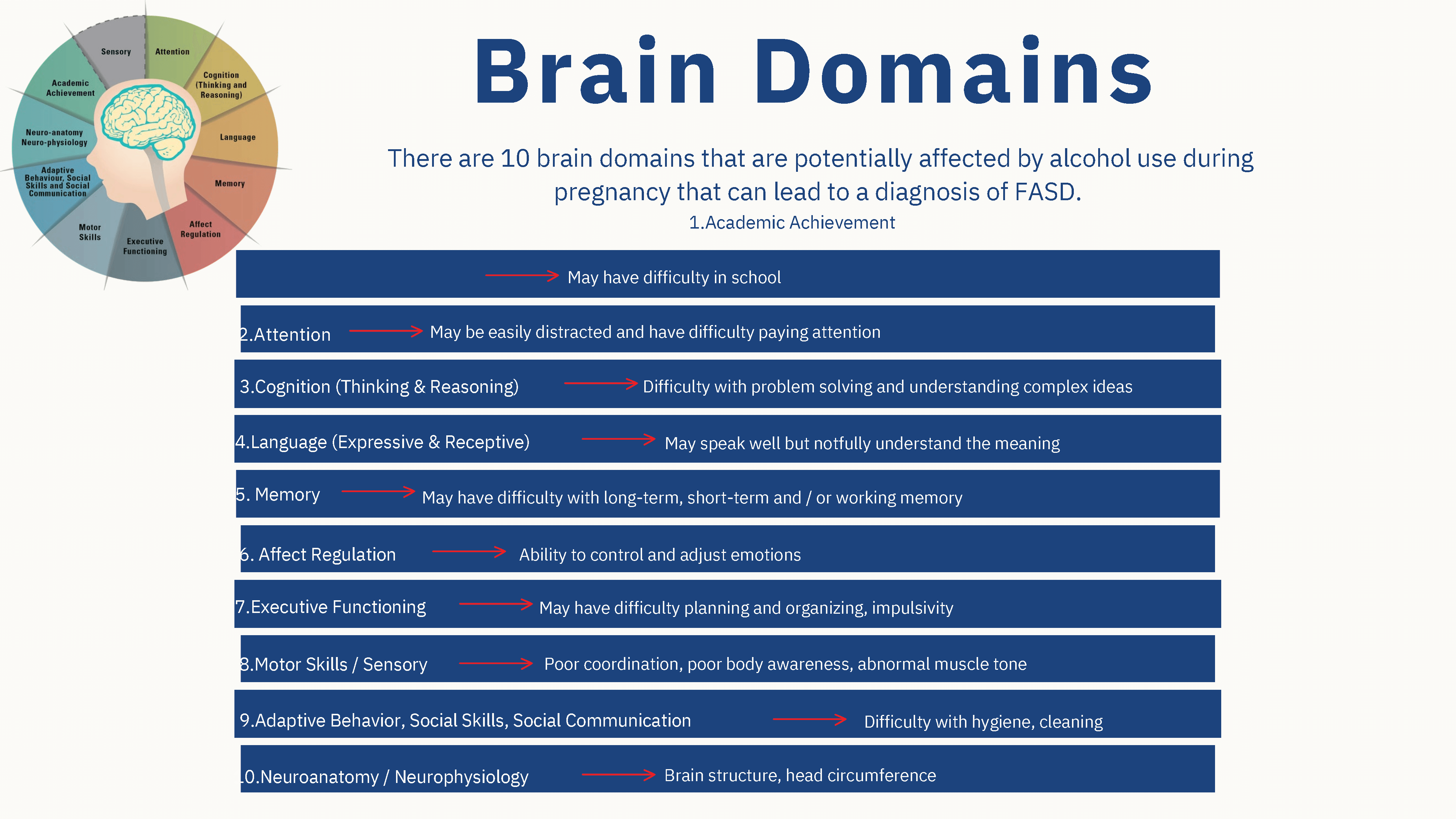
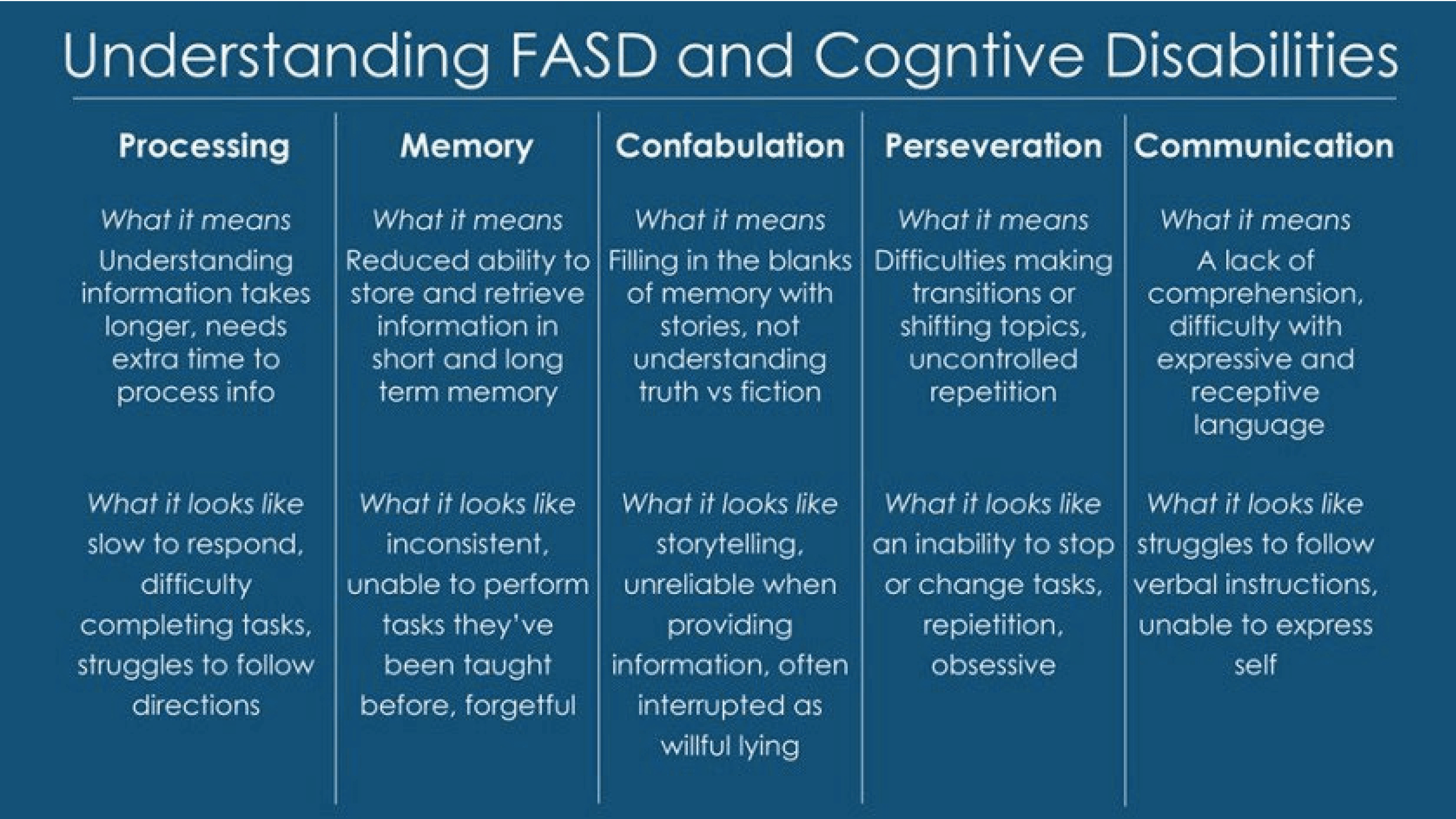
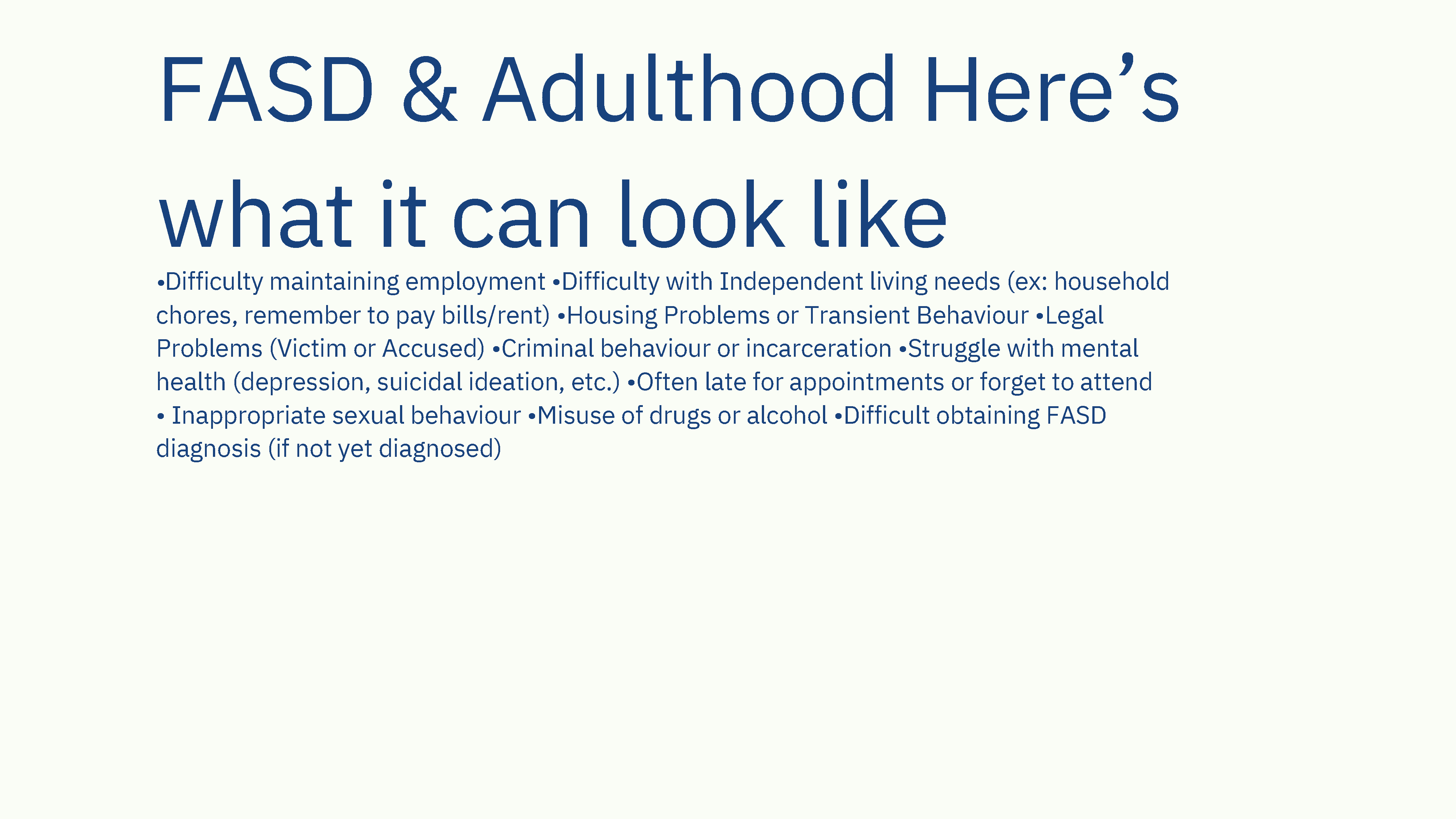
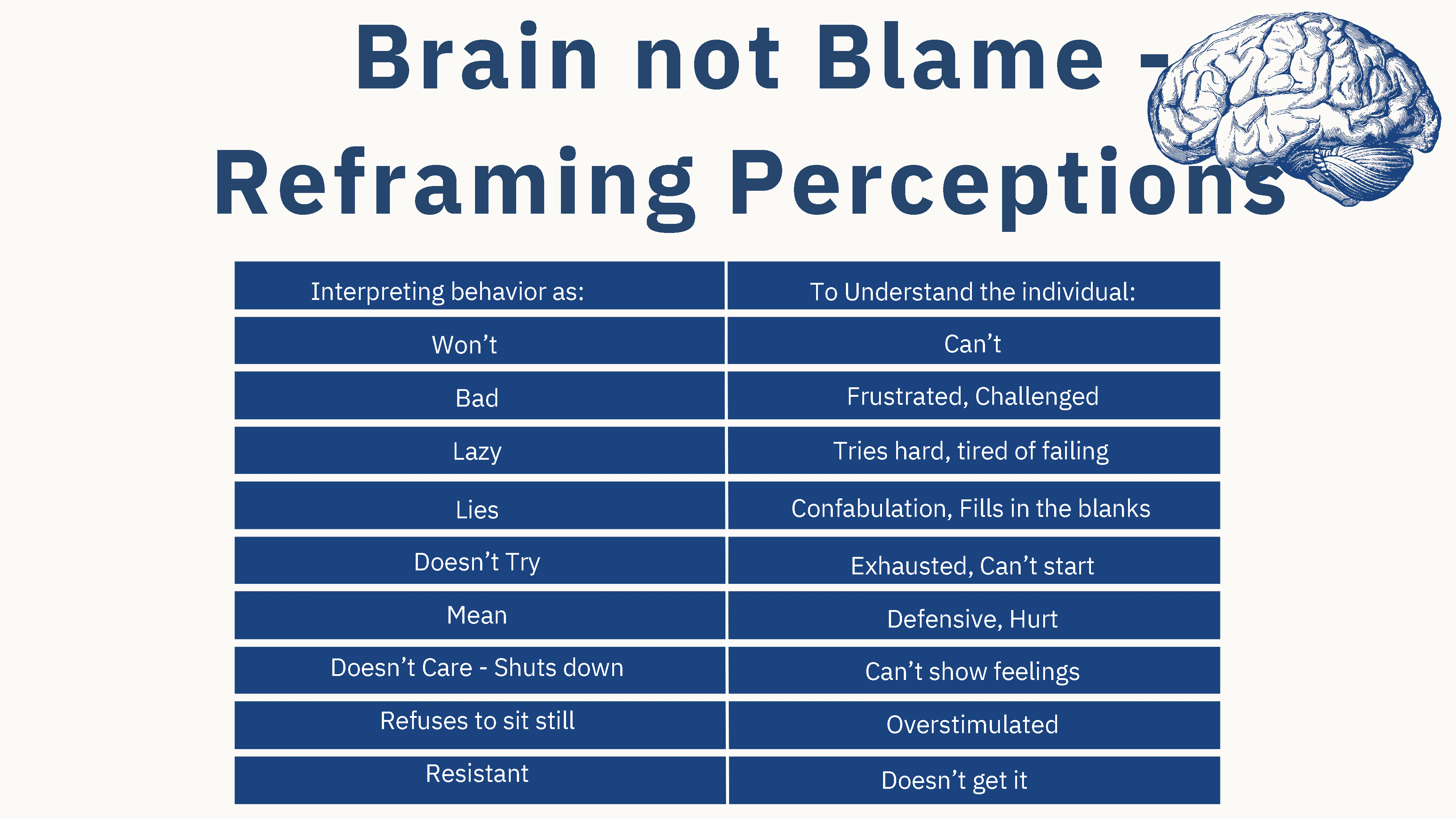
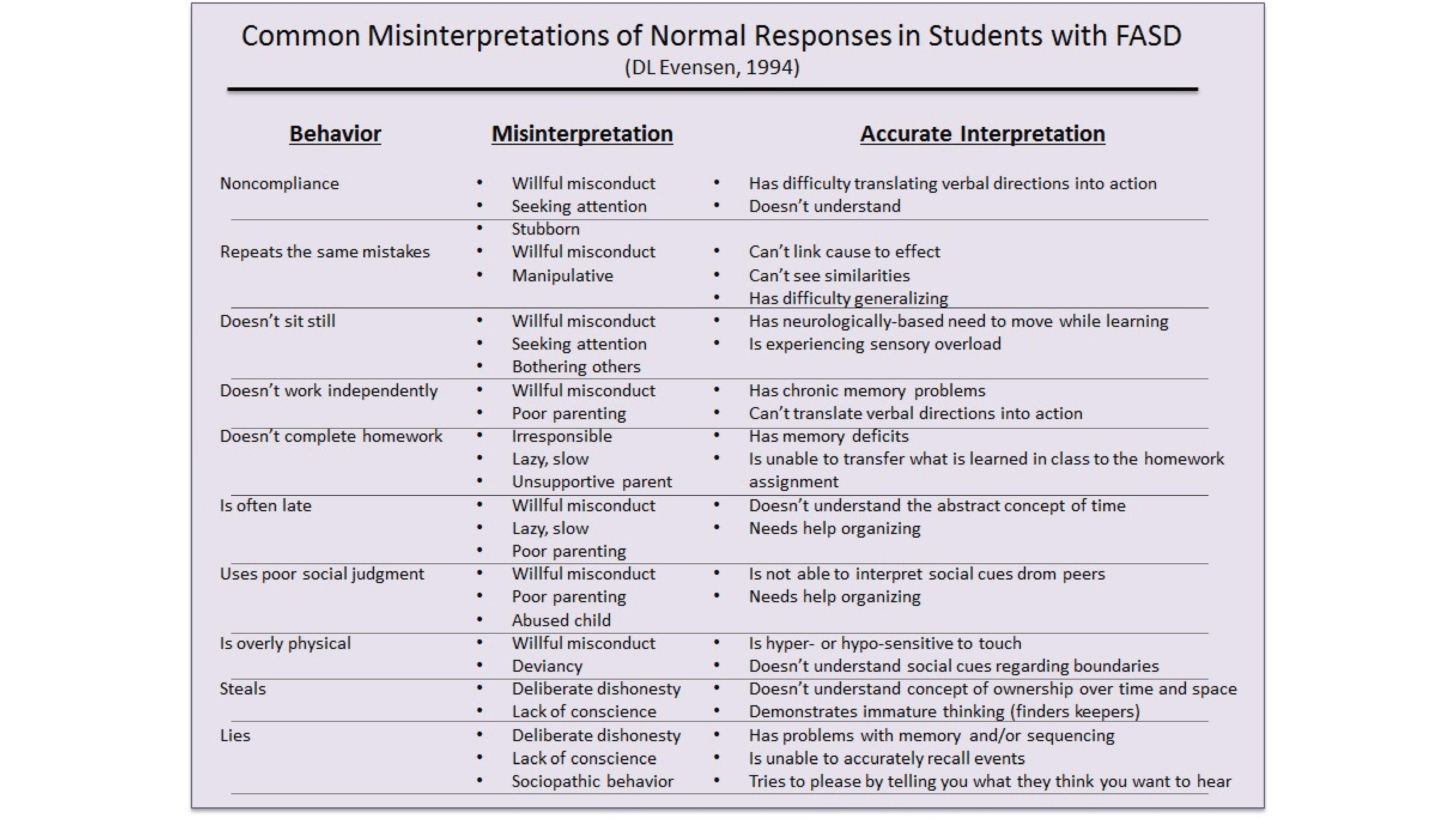
FASD – Fetal Alcohol Spectrum Disorder. (n.d.). Cochrane Temiskaming Children’s Treatment Centre. Attached
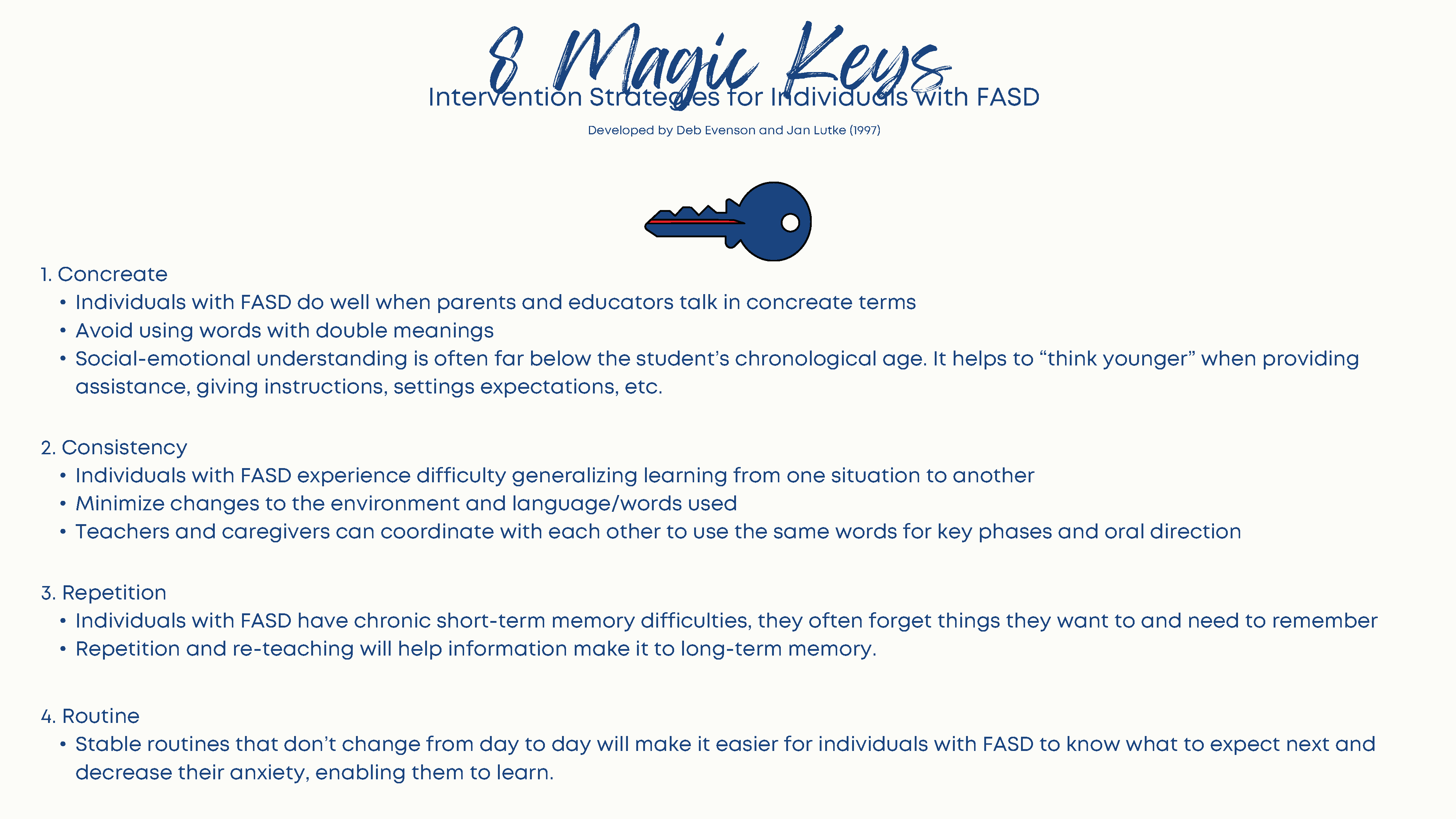
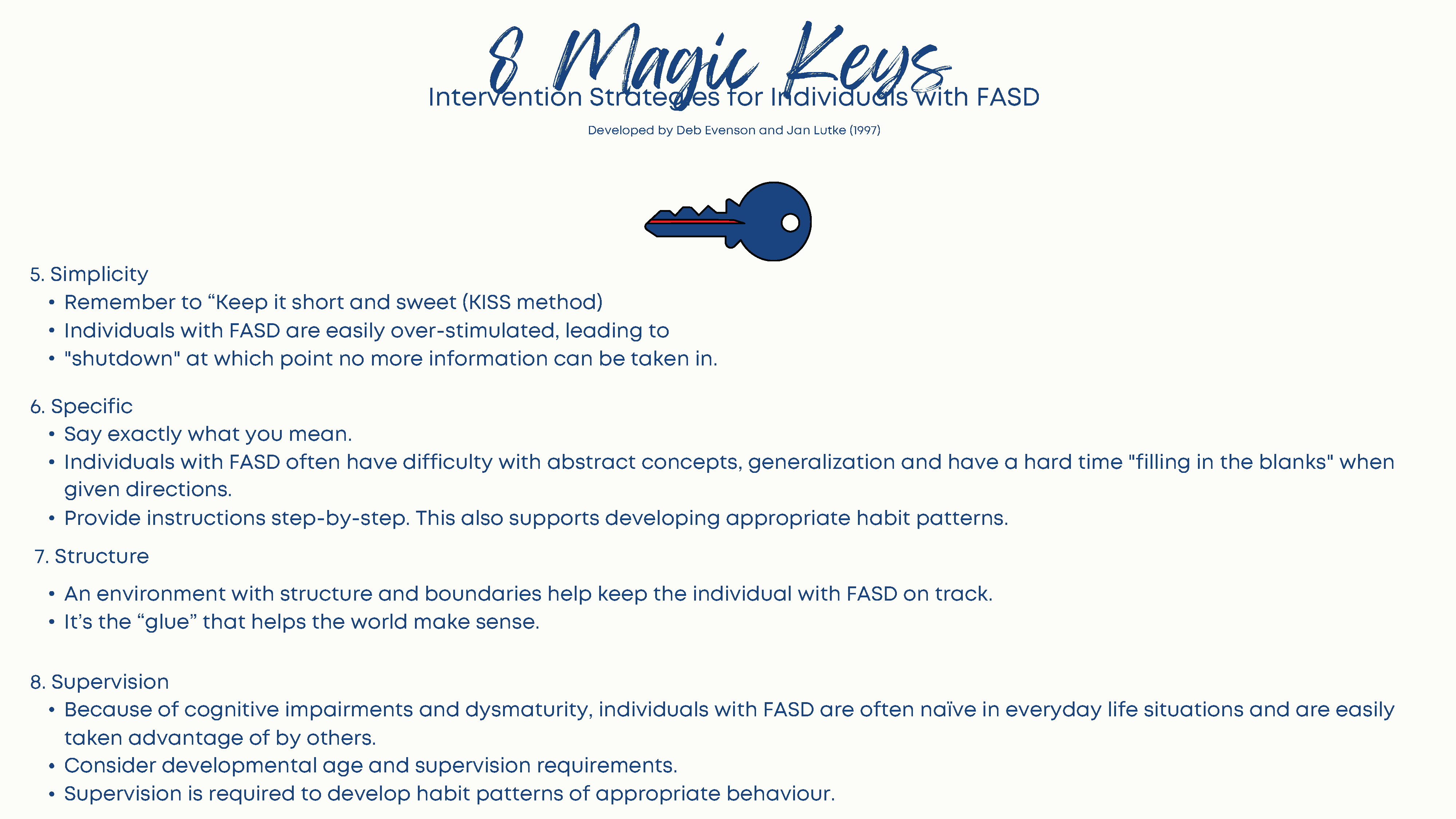
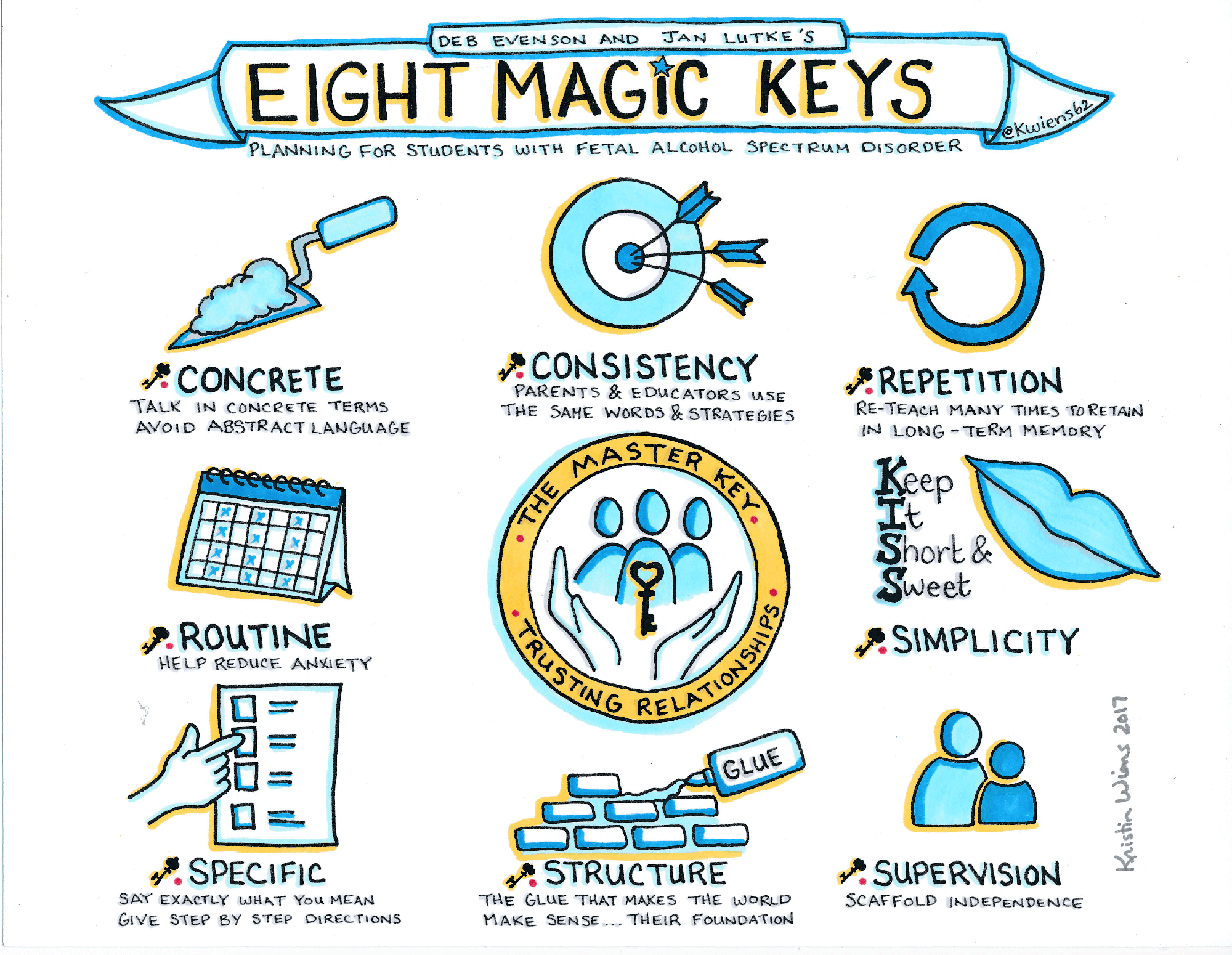
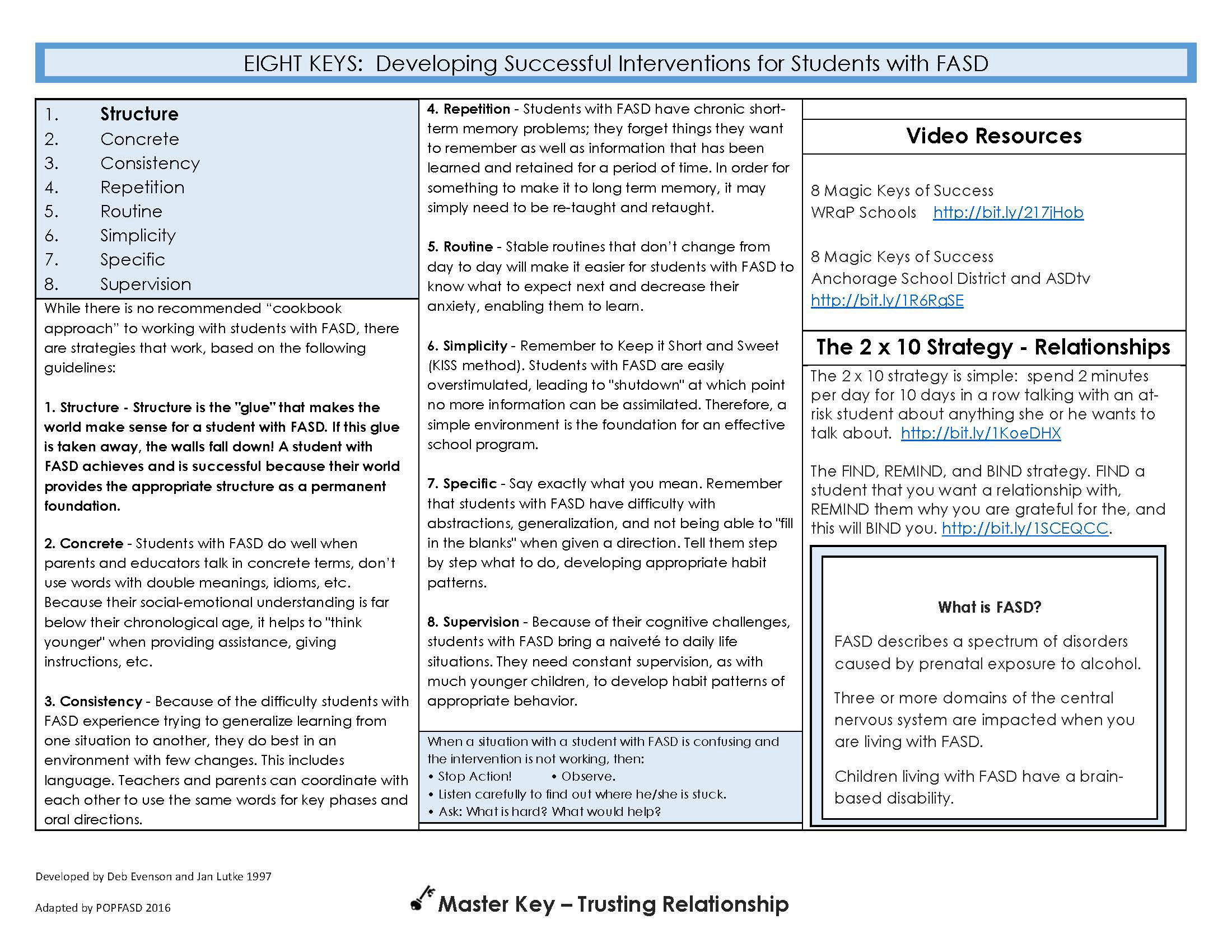
Eight Magic Keys – Planning for Students with Fetal Alcohol Spectrum Disorder.
(1997). Evenson, D. & Lutke, J., Attached


What’s Fragile X Syndrome (FXS)?
Fragile X syndrome (FXS), also known as Martin-Bell syndrome, is the most common cause of inherited intellectual disability. FXS is caused by a change in a gene on the X chromosome. This change means the body cannot make a protein needed for normal brain development.
Facts about FXS
There are not always interventions for the below symptoms, however, seeing a decrease/absence of symptoms may indicate if a patient/client’s medications are working.
It can lead to:
People with FXS also may have other conditions, including:
Students with FXS may:
What Workers Can Do
Individuals with FXS work best in a calm, structured learning environment without distractions.
References:
Gavin, M. L. (2020, September). Fragile X syndrome factsheet (for Schools) (for parents) – nemours kidshealth. KidsHealth.
Generalized anxiety disorder is chronic anxiety, with symptoms occurring for at least 6 months. A person with GAD has excessive worry that is difficult to control. It impairs work, ability to sustain relationships, and daily functioning. It is twice as common in the female population than it is for the male population.
| Symptom | Presentation | Presentation Intervention |
|---|---|---|
| Fatigue | Feeling easily tired | Encourage sleep hygiene, adequate nutritional and fluid intake. Refer to dietician if needed |
| Concentration and restlessness | Difficulty concentrating or patient's mind going blank. Pacing, inability to stay still | Grounding, and mindfulness. Refer to psychologist or CBT programming if available |
| Irritability | Being easily agitated | Encourage client to attend to enjoyable activities - refer to recreational therapist |
| Muscle tension | Feeling stiff | Relaxation techniques, meditation |
| Sleep | Sleep disturbance (difficulty falling or staying asleep, restless, unsatisfying sleep) | Encourage routine meals, and sleep schedule |
Interventions for all Anxiety Disorders
Treatment for GAD
If the GAD disorder is mild, no treatment may be required, and the physician may follow up every 3 months to observe for any worsening symptoms.
If treatment is required, cognitive behavioral therapy (CBT) can be used as treatment on its own, or in combination with medication (selective serotonin reuptake inhibitors or serotonin-norepinephrine reuptake inhibitors).
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Generalized Anxiety Disorder (GAD). Ontario Tech University.
Intellectual disability is a developmental disability. It can affect people in different ways and at different levels. Intellectual disability is a life-long condition. There are three criteria that need to be identified to provide a diagnosis.
1. The individual’s general intelligence needs to be developing/or have developed at a slower rate.
This can be seen through difficulties at school, special education classes, etc.
2. There needs to be significant difficulties in the individual’s everyday living skills.
Difficulty maintaining employment, social skills, communication, selfcare, self-direction, home living, functional academics, etc.
3. Challenges with intelligence and everyday living skills prior to age 18.
If working with an adult, the difficulties listed above must have been noted in early life
Causes
There are many causes of intellectual disability; however, sometimes the causes may be unknown. Some causes are:
Different Severities of Intellectual Disability
Intellectual disability has four different severities. The most common severity of intellectual disability is “mild”. People with intellectual disability in the mild range learn at a slower rate but with early intervention and support from adults throughout their childhood and early adulthood, can live an independent or semi-independent life. They may graduate high school, have relationships, or maintain a job.
“Moderate”, “severe”, and “profound” are the other severities of intellectual disability. These are less common but usually make it harder for the individual to live an independent life.
Supporting someone with Intellectual Disability
Everyone is different and intellectual disability can affect everyone differently. Therefore, individualized plans and getting to know how the individual learns are important in supporting them the best way possible. Listed below are some general strategies for supporting individuals with intellectual disabilities.
References:
Do2Learn. (1999-2021). Intellectual Disability, Strategies. Do2Learn.
What are Mood Disorders?
Before we get into the clinical details, remember that patients/clients may have no control of their own behavior/speech, so it is important to always take your time, and be patient when caring for them. Keep in mind that they may not be in a state to fully appreciate what you are saying now, and they will not forget how you made them feel.
Mood Disorders are a class in mental illness that broadly encompasses various types of bipolar disorders and depression. This disorder can affect all ages of patients/clients, where the symptoms of mood disorders may be expressed differently by each age group.
Major Depressive Disorder
Major depressive disorder (otherwise known as depression), is a common and recurring mood disorder that impacts a person’s daily functioning. The World Health Organization (WHO) ranks major depression as the 11th cause of disability and mortality.
| Symptom | Presentation | Intervention |
|---|---|---|
| Depressed Mood | Depressed mood most of the day (e.g., feels sad, empty, hopeless) or observed by others (e.g., appears tearful). In children and adolescents, it may display as irritable. | Observe and assess for fluctuations in mood, worsening mood. Document in MSA/MSE, and in progress note. |
| Diminished Interest | No longer interested in any activities. | Encourage client to attend recreational groups and activities, even if it's passive participation. Connect with a recreational therapist for client-centered activities. |
| Weight loss | Significant weight loss, weight gain, or change in appetite. | Collaborate with a dietician to increase caloric intake, provide food or beverages that interest client. |
| Insomnia / Hypersomnia | Insomnia: difficulty falling asleep, waking up too early, waking up in the middle of the night, difficulty paying attention. | Assist with providing good sleep hygiene.
Maintain routine times of waking up, going to bed, and regular timed meals. Connect with an occupational therapist. Advocate for and provide medication to aid with sleep. Provide medication if all other non-pharmacological interventions are not effective. |
| Psychomotor Agitation | Psychomotor agitation, slow speech, slow movement, slow thought processes. | Staff should allow adequate time to accommodate for slow movement and thought processes. Use of de-escalation techniques, distraction, and redirection if client becomes agitated. Offer medications if nonpharmaceutical methods do not reduce agitation. |
| Fatigue | Fatigue or loss of energy. | Encourage adequate food and fluid intake, low impact exercise or mobility. |
| Worthlessness / Guilt | Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional). | Provide validation for emotions and support. Connect with a psychologist or advocate for referral to psychotherapy/CBT programming. Build therapeutic relationships and rapport. Use positive affirmations change negative thinking processes. It is easier to change negative thinking processes if you have a therapeutic relationship and rapport with the client. |
| Lack of concentration / Indecisiveness | Diminished ability to think or concentrate, experiences indecisiveness. | Be mindful of the client's limitations at this time; providing patience, dignity, and respect. Be clear and speak slowly during interactions. Repeat important information. Provide frequent reminders. |
| Suicidal Thoughts | Recurrent thoughts of death, suicidal ideation, suicide attempts. | Perform daily or more (depending on facility’s policies and client acuity) suicide risk assessment. Observe any
environmental safety concerns, remove items that pose a risk. May need to advocate to increase observation depending on suicide and self-harm risk. |
Interventions for Depression
Treatment for Depression
Treatment for Depression: Psychotherapy
Cognitive behavioural therapy (CBT) is a psychotherapeutic treatment originally developed for depression. It is assumed that behaviour is mediated by one’s thoughts. Therefore, changing the behaviour will affect one’s thoughts, and vice versa. The goal of CBT is to change a person’s negative thought process.
Treatment for Depression: Pharmacology
Antidepressants, typically Selective Serotonin Reuptake inhibitors (SSRI), are prescribed for depression. If one medication is not effective, the physician trials another, until one of the medications improves depression symptoms with the least side effects.
Antidepressants in general take 2-6 weeks to observe any improvements in mood.
Types of medications for major depressive disorder:
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Major Depressive Disorder. Ontario Tech University.
Obsessions or compulsions are time-consuming (e.g. they take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
*It is important to note that OCD symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition.
Obsessions:
Compulsions:
| Symptom | Presentation |
|---|---|
| Intrusive thoughts (obsessions) | Recurrent and persistent thoughts, urges, or images that are unwanted, and causing high levels of anxiety. |
Interventions for Depression
Treatment for Depression
Treatment for Depression: Psychotherapy
Cognitive behavioural therapy (CBT) is a psychotherapeutic treatment originally developed for depression. It is assumed that behaviour is mediated by one’s thoughts. Therefore, changing the behaviour will affect one’s thoughts, and vice versa. The goal of CBT is to change a person’s negative thought process.
Treatment for Depression: Pharmacology
Antidepressants, typically Selective Serotonin Reuptake inhibitors (SSRI), are prescribed for depression. If one medication is not effective, the physician trials another, until one of the medications improves depression symptoms with the least side effects.
Antidepressants in general take 2-6 weeks to observe any improvements in mood.
Types of medications for major depressive disorder:
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Major Depressive Disorder. Ontario Tech University.
Definition: ODD is a behaviour disorder in which a person displays a pattern of angry or irritable mood, defiant or confrontational behavior, and vindictiveness toward people in
authority. The exact cause of ODD is not known, but a combination of biological, genetic, and environmental factors may contribute to the condition.
Common behaviours:
Provide Choice
Demands may be better received if they are presented as a choice rather than a direct instruction. In this way, the client experiences an opportunity for control without having to engage in challenging behaviours. For example:
Avoid Power Struggles (‘Time In’)
Transitions (Changing from one activity to the next)
References:
K. Barloso, Autism Parenting Magazine. Oppositional Defiant Disorder Treatment Plan (October 18, 2023). Accessed at:
https://www.autismparentingmagazine.com/oppositional-defiant-disordertreatment/
Mayo Clinic, Oppositional defiant disorder (ODD) (January 4, 2023). Accessed at:
ODD: A Guide for Families by the American Academy of Child and Adolescent Psychiatry: Oppositional Defiant Disorder (2009). Accessed at
https://www.aacap.org/App_Themes/AACAP/docs/resource_centers/odd/odd_resource_center_odd_guide.pdf
When a person has recurring rapid attacks of intense anxiety, fear, and discomfort that becomes debilitating.
The table below outlines the major symptoms and appropriate nursing interventions:
| Symptom | Presentation | Intervention |
|---|---|---|
| Fear | Sweating, fear of losing control, fear of dying, restlessness. | Teach coping skills or strategies when patient/client is not in a heightened emotional state. Remind client of these strategies when in a heightened state. Provide privacy, decrease stimuli. |
| Derealization or depersonalization. | Patient feels detached from surroundings | During interaction, you may need to speak loudly, clearly, and slowly. You may need to repeat sentences multiple times. |
| Physiological Symptoms | Paresthesia, feeling dizzy/unsteady/lightheaded/faint, trembling, shaking, palpitations, shortness of breath, smothering, chest pain or discomfort, nausea, abdominal discomfort. | Use grounding techniques such as providing ice for bodily comfort, focus on the moment (mindfulness). Model deliberately slow breathing exercise to reduce physiological symptoms. Offer medication for anxiety if available and necessary. |
Treatment for Panic Disorder
Best practice treatment is:
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Panic Disorders. Ontario Tech University.
Definition: Pica is an eating disorder where a person persistently eats or craves things that are non-food items. The behaviour must be present for more than a month, developmentally inappropriate or not culturally practiced. Items that are commonly eaten are: glass, paint chips, clay, cigarette butts, hair, feces, dirt, coins, ice, paper, grass, rocks, plaster and toys. Pica is not limited to this list and almost anything could be consumed.
Common health concerns:
Supporting someone with Pica:
References:
Autism Speaks Autism Treatment Network, Autism Speaks, & Massachusetts General Hospital.
(2014). Pica (p. p.1-1). https://thompsoncenter.missouri.edu/wpcontent/
uploads/2016/11/PICA-PROFESSIONALS-GUIDE_FINAL.pdf
George Timlin and Joanna Burden. (2017). PICA Information Sheet.
https://www.sendsupported.com/wp-content/uploads/2017/09/PICA-doc.pdf
PICA – National Eating Disorders Association. (2024, March 22). National Eating Disorders
Association.
https://www.nationaleatingdisorders.org/pica/
Pica (eating non-edible items). (2023, November).
https://www.cambspborochildrenshealth.nhs.uk/services/cambridgeshire-communitypaediatrics/
pica-eating-non-edible-items/
Definition: This is a rare genetic condition in which the person has a constant sense of hunger. They want to eat constantly because they never feel full (hyperphagia). Many of the health complications that persons with Prader-Willi syndrome have are due to obesity.
Common signs and behaviours:
Behaviour Intervention Strategies
References:
National Organization for Rare Disorders. Prader-Willi Syndrome (July 12, 2023)
Accessed at: https://rarediseases.org/rare-diseases/prader-willi-syndrome/
Prader-Willi Syndrome Association. Applied Behaviour Analysis and Prader-Willi
Syndrome, Part 1: Explaining ABA (October 3, 2018). Accessed at: https://www.pwsausa.org/applied-behavior-analysis-and-prader-willisyndrome-
part-1-explaining-aba/
What is Schizophrenia?
Schizophrenia is defined as a psychiatric disorder involving chronic psychosis. Little is known on what causes Schizophrenia, however, researchers believe that it may be a combination of the individual’s brain chemistry, family disposition and environmental contributors.
Symptoms of Schizophrenia
There are not always interventions for the below symptoms, however, seeing a decrease/absence of symptoms may indicate if a patient/client’s medications are working.
Positive Symptoms:
A change in behavior/thought which is observably present in a patient. These are delusions, hallucinations, and disorganized speech.
1.) Delusions
Described as fixed false beliefs; not culturally sanctioned, intensity can vary, described as though it exists.
Persecutory/paranoid: believes one is in danger, being followed/monitored, harassed/conspired against. May involve a government agency/family/neighbours/friends. If paranoid, they believe they will be harmed by others and will be exhibited by suspiciousness (ex. Need all food items to be unopened
in order to take their medications)
Referential
Grandiose: patient believes that they have a special power/talent/abilities/identity (ex. They believe they are God)
Thought broadcasting/insertion/withdrawal
2.) Hallucinations
3.) Disorganized Speech
Disorganized speech is indicative of disorganized thought process. This means that it’s hard to follow a patient/client’s train of thought or be able to respond coherently to
questions asked.
Negative Symptoms:
Negative symptoms are functions that have been diminished or are not present in the patient.
1.) Lack of Motivation
2.) Diminished emotional expression
3.) Apathy
4.) Lack of energy
Treatment for Schizophrenia
Antipsychotic medications are part of the main line of treatment for individuals with schizophrenia, along with Cognitive Behavioral Therapy (CBT) in helping with residual
symptoms. The family/caregiver should also be provided support as Schizophrenia is a lifelong illness.
Inpatient Treatment:
Outpatient Treatment:
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Schizophrenia. Ontario Tech University.
Social Anxiety Disorder refers to a high level of anxiety/fear during or around social situations.
The table below outlines the major symptoms and appropriate interventions:
| Symptom | Presentation | Intervention |
|---|---|---|
| Avoidance of Social Situations | Tries to leave social situations before or while they occur. | Promote participation, can be passive participation in group programming. Provide exposure and routine to social situations. Promote use of items that may distract the client during social situations, such as an item that can be used as a fidget device. |
| Fear and feelings of anxiety | They fear that anxiety symptoms that will be negatively evaluated, and lead to rejection by others. | Assist by changing negative cognitive constructs to positive ones. For example, if voicing thoughts that people are not enjoying their company, you can say that their company has been pleasant. |
Treatment for Social Anxiety Disorder
Treatment may fall between Cognitive Behavioural Therapy (CBT) and/or medication (SSRI or SNRI) for initial therapy, based on availability and patient preferences.
References:
Ontario Shores Foundation for Mental Health (2023). Common Mental Illnesses:
Assessment and Documentation. Social Anxiety Disorder. Ontario Tech University.
Please find below the following resources for this section:
HANDS & Vita CLS – The international Journal for Direct Support Professionals:
Volume 9 – Issue 3 – March 1, 2020 (6 pages)
References:
The international Journal for Direct Support Professionals. Volume 9 – Issue 3.
(March, 2020). HANDS & Vita CLS. Attached
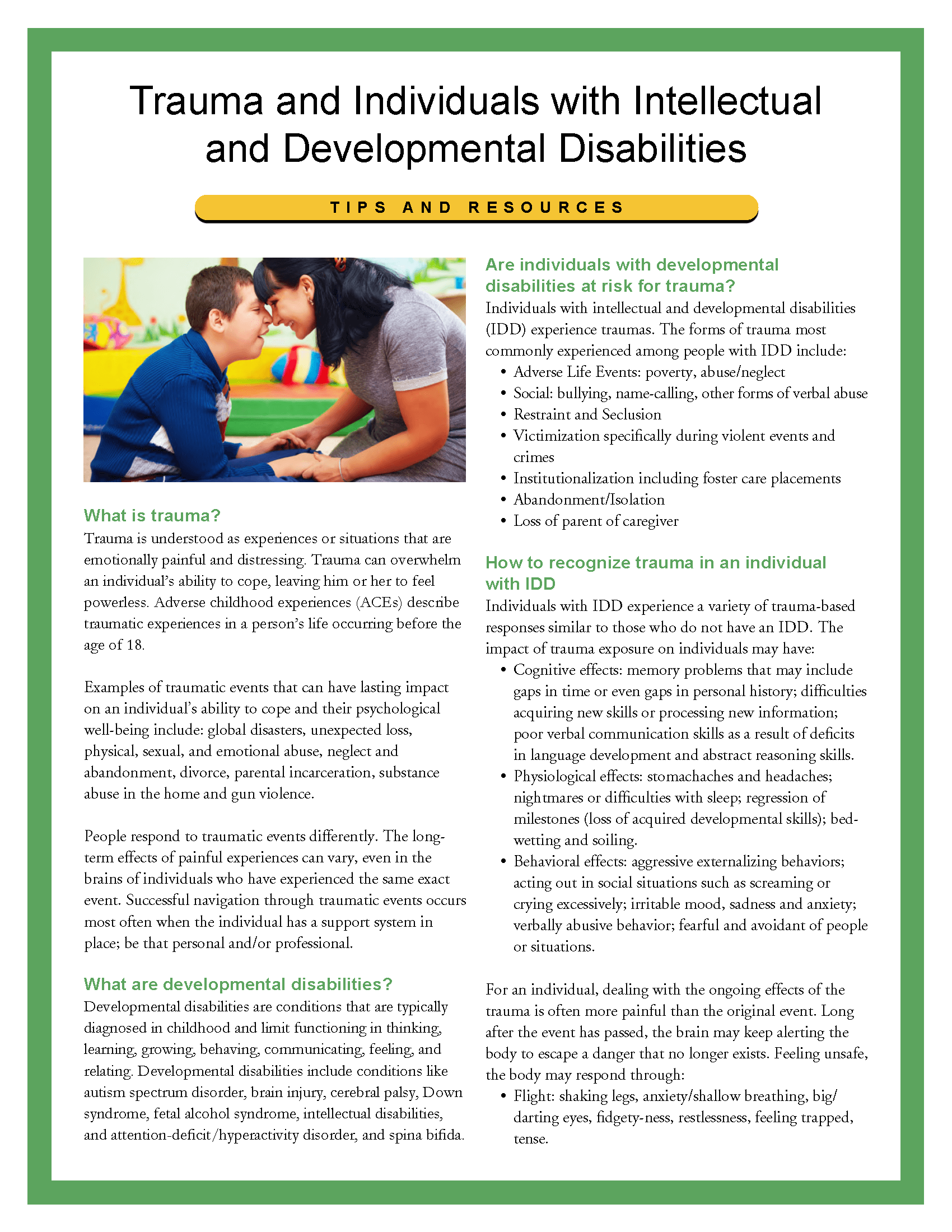
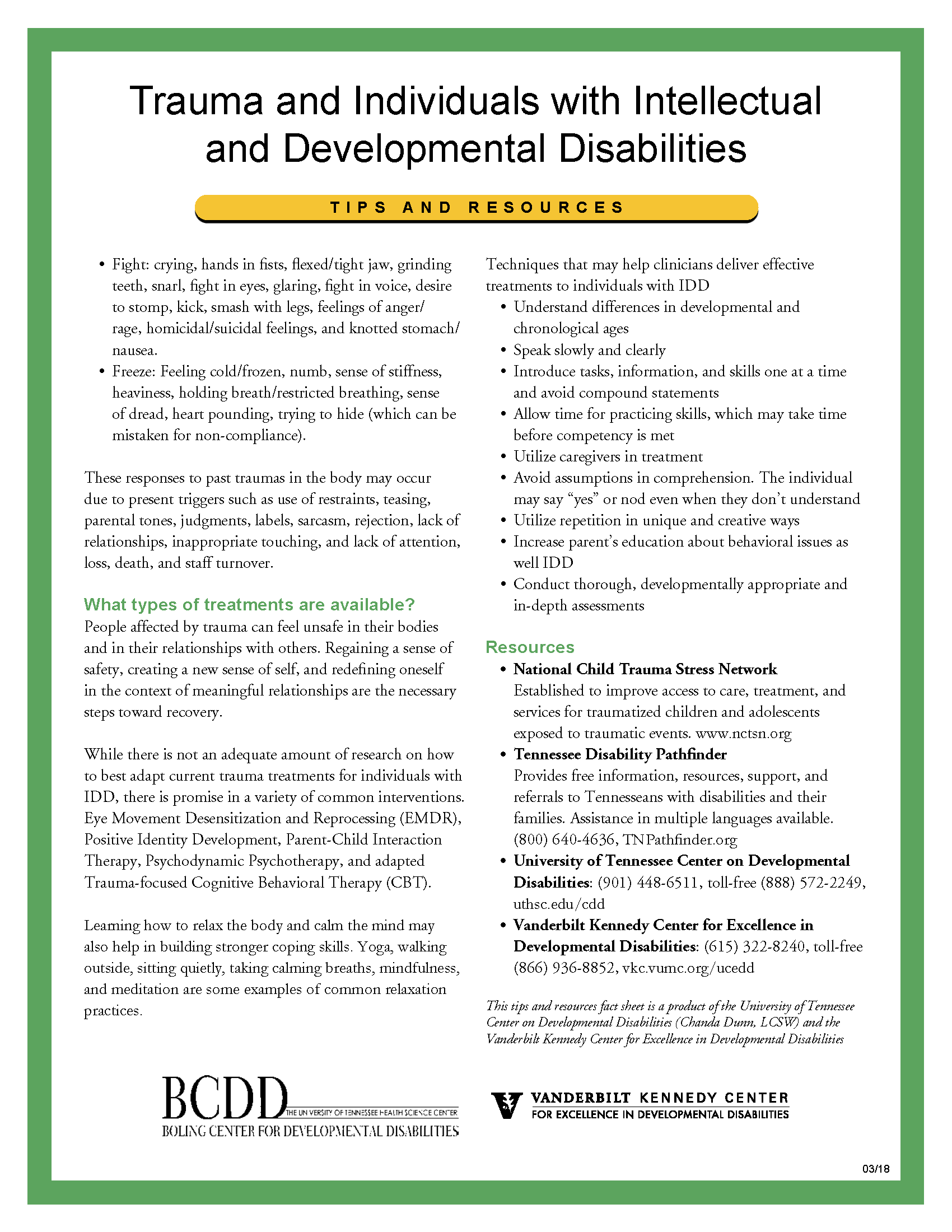
Please find below the following resources for this section:
References:
Chanda Dunn. (2018). Trauma and Individuals with Intellectual and Developmental
Disabilities. University of Tennessee Center on Developmental
Disabilities, Vanderbilt Kennedy Center for Excellence in Developmental Disabilities.